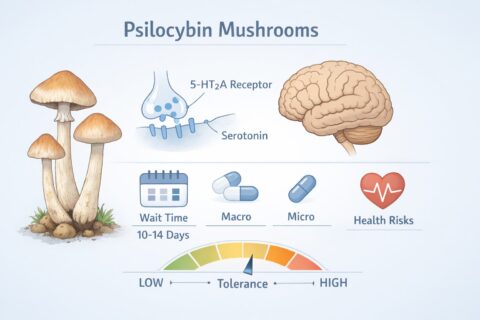
Psilocybin, the active compound found in certain mushroom species, is the subject of ongoing research into its possible mental health benefits. When consumed, psilocybin converts to psilocin in the body, which interacts with serotonin receptors in the brain. This can lead to changes in perception, mood, and awareness.
Although there is growing interest in the study of psilocybin, it remains a controlled substance in both Canada and the United States. Its use is only permitted through approved clinical trials or limited medical exemptions. This article is for informational and educational purposes and reviews observed patterns of psilocybin use as documented in research settings and non-clinical reports.
Researchers and participants often refer to two types of psilocybin use:
Each type is associated with different patterns of frequency and different sets of risks.
Macrodosing involves a moderate to high intake of psilocybin and is associated with strong changes in perception, emotions, and awareness. In clinical research, macrodoses are used under professional supervision, with careful screening and monitoring.
Observed Frequency in Research
Studies generally space macrodose sessions far apart: typically 2 to 4 weeks or more. This interval allows time for psychological integration and reduces the likelihood of physical tolerance.
Physiologically, the body becomes less responsive to psilocybin after frequent use. If taken on consecutive days, the effects quickly diminish. This built-in tolerance response discourages repeated high-dose use.
Microdosing refers to very small doses of psilocybin that do not cause noticeable psychedelic effects. While formal scientific evidence is limited, anecdotal reports suggest that some individuals use microdoses in efforts to improve mood, focus, or creativity.
Observed Patterns (Non-Clinical Sources)
In non-clinical literature, various self-administered schedules have been documented. These typically involve alternating days of use and rest, with the intent of avoiding tolerance buildup. These patterns are not medically approved or standardized and should not be considered treatment plans.
It is difficult to define exact dosing standards because mushroom potency varies based on species, growing conditions, and preparation methods.
The following table summarizes general dose ranges documented in historical, user-reported contexts. This information is presented for public education and is not a guide for self-use.
| Dose Level | Dried Mushroom Weight | Observed Effects |
| Low to Moderate | 1.0 – 2.5 grams | Mild changes in perception, introspection |
| Standard to High | 2.5 – 3.5 grams | Intense visuals, altered sense of time/self |
| Very High | 5.0 – 6.0 grams | Overwhelming psychological effects (rare use) |
In clinical trials, a standard dose may be around 25 mg of pure psilocybin, which is roughly equivalent to 2.5 grams of dried Psilocybe cubensis. However, the natural form varies widely, which is why accurate measurement and caution are important in research environments.
| Dose Level | Dried Mushroom Weight | Observed Effects |
| Microdose | 0.1 – 0.2 grams | No hallucinations; subtle effects |
Microdosing, when studied, is intended to produce no noticeable psychedelic effects and should not cause cognitive impairment.
While psilocybin is not known to be physically toxic, studies and case reports have identified risks that are important to understand, especially in cases of high or repeated exposure.
Clinical studies consistently emphasize the importance of set (a person’s mental state) and setting (the physical and social environment). These two factors can greatly influence the nature of a psychedelic experience.
This is why psilocybin sessions in research are often held in structured, quiet rooms with trained professionals present.
Across clinical trials and expert recommendations, the following best practices are often observed:
Psilocybin remains under federal control in both Canada and the United States. Legal access is limited to regulated clinical trials and medical exemptions. However, public interest and research continue to grow.
By reviewing the scientific literature and observed use patterns, we gain a better understanding of how frequency, dose, and setting influence both the potential benefits and risks of psilocybin. Ongoing studies aim to explore whether this substance can play a role in mental health treatment, but caution, structure, and medical oversight are essential.
If you are exploring this topic from an academic or health policy perspective, always consult peer-reviewed sources and recognize that findings in research settings may not apply outside those controlled environments.
© 2025 All rights Reserved.
Rocket Mushroom Shop

Are You 18 Or Over?
By clicking 'Continue', you confirm that you are over 18 years old. By using this website, you agree to our terms of service.